What about all the Media Claims that there is Scientific Evidence that Social Isolation Works???
Here are some typical claims made by the Mass Hysteria Media:
“There is plenty of scientific evidence to support the use of social distancing.
“Numerous studies have demonstrated that social distancing measures can be very effective in slowing the spread of respiratory viruses and reducing the number of people who ultimately get infected.”
“Social distancing can flatten the curve and reduce the strain on our medical system.”
Sadly, almost never do any of these claims link to any scientific study that supports the claims they are making. When they do link to a study, it is often the discredited 2020 Ferguson study or the discredited 2007 Ferguson study.
While there has not been a single credible scientific study that actually shows that Social Isolation works, there are almost every day, a new wave of fake science studies claiming that social isolation works. These fake science studies are then promoted by the Mass Hysteria Media to help keep folks locked up in their houses. In this section, we will take a closer look at a few of these fake science studies with the hope that it will help you better understand the difference between real science and fake science.
Now for our lineup of fake science articles.
#1 Our first fake science article is called Pandemics Depress the Economy, Public Health Interventions Do Not.
Here is a link to this article: https://papers.ssrn.com/sol3/Papers.cfm?abstract_id=3561560
The article is 40 pages long.
Red Flag #1 is that the authors of this article work for the US Federal Reserve Bank. The purpose of the article is to reassure the public that the economy is not being destroyed by the current extreme social isolation policies (despite the fact that more than 30 million jobs have been lost in just the past 6 weeks) - and that social isolation policies are working to stop the corona virus. To prove their point, they looked at social isolation efforts made by 43 cities during the 1918 Spanish Flu epidemic.
Red Flag #2 is that they referred to the discredited Ferguson 2007 study.
Red Flag #3 is their claim that more aggressive social isolation policies not only saved lives – but also led to improved economic performance after the pandemic was over. Here is a quote from the study: “We find that cities that intervened earlier and more aggressively do not perform worse and, if anything, grow faster after the pandemic is over. Our findings thus indicate that NPIs not only lower mortality; they may also mitigate the adverse economic consequences of a pandemic.”
Perhaps the most important chart in the entire study was a chart showing that the Spanish Flu and Pneumonia fatalities during the 1918 epidemic were directly related to the Pneumonia fatalities the year before in 1917. Here is the chart:
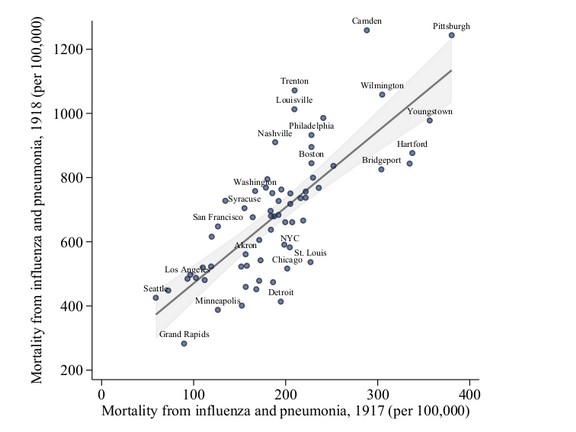
Although the authors of the study did not realize it or attempt to explain this chart, the reason there was a relationship between city location and illnesses is that some cities have better air quality and more healthy people with better immune systems than other cities. It is also obvious from the above chart that we could predict Spanish Flu fatalities in 1918 simply by multiplying the 2017 pneumonia fatalities times three. In other words, the 1918 Spanish Flu fatalities had nothing to do with the social isolation policies of each city and instead had to do with the immune systems of the populations in each city. In short, the above graph is strong evidence that the claim they attempt to make in their study is false. I think anyone with a pair of eyes and a couple of functioning brain cells can see that.
Did I mention that the Federal Reserve is not part of the federal government – and that it has no reserves? What it really represents are Wall Street banks!
The moral here is to always look at the actual data rather than what the authors are saying about the data. This concludes our first fake study. Now on to the next one.
#2 Our next fake science article, released in April 2020, was called: “Nonpharmaceutical Measures for Pandemic Influenza in Non healthcare Settings—Social Distancing Measures”
This article was a review of 50 scientific studies which supposedly confirmed the effectiveness of social distancing policies in minimizing the spread of flu epidemics. Here is the link so you can read it yourself. https://wwwnc.cdc.gov/eid/article/26/5/19-0995_article
Here was the ending of their abstract:
“We conducted systematic reviews of the evidence base for effectiveness of multiple mitigation measures: isolating ill persons, contact tracing, quarantining exposed persons, school closures, workplace measures/closures, and avoiding crowding. Evidence supporting the effectiveness of these measures was obtained largely from observational studies and simulation studies. Voluntary isolation at home might be a more feasible social distancing measure, and pandemic plans should consider how to facilitate this measure. More drastic social distancing measures might be reserved for severe pandemics.”
As I had not seen a single study supporting the effectiveness of social distancing, I looked forward to reading the 50 studies. Sadly, 21 of the so-called studies were simply computer simulations where they assumed social distancing worked and then found that their computer model agreed with their assumption. What a surprise. I want to make it clear that computer simulations should NEVER be lumped together with real scientific studies.
The remaining 29 observational studies actually refuted the contention that social distancing worked.
Here was a Table of the 50 studies divided by type of intervention.
|
Type of NPI |
# studies |
study design (1) |
Main Findings |
|
Isolation |
15 |
4 O 11 S |
Isolation has moderate impact in reducing influenza transmission and impact. |
|
Quarantine |
16 |
1 I 5 O 10 S |
Quarantine has low impact in reducing influenza transmission and impact. |
|
Contact Tracing |
4 |
4s |
contact tracing provides only modest benefit but will need substantial resources. |
|
School Closure |
--- |
--- |
see three types below |
|
Planned holiday |
28 |
o |
transmission of influenza decreases during routine school holidays but increases after schools reopen. |
|
reactive closures |
16 |
o |
The effectiveness of reactive school closure varies. |
|
pre-emptive closures |
13 |
o |
Preemptive school closure has moderate impact in reducing influenza transmission. |
|
Workplace closure |
10 |
s |
Workplace closures has only modest impact in reducing influenza transmission. |
|
Avoiding crowds |
3 |
o |
Timely and sustained application of measures to avoid crowding might reduce influenza transmission. |
|
Total |
50* |
29-O 21S |
|
*Some studies had results in more than one category.
(1) O = Observational, I = Intervention S = Simulation
Here is a quote from the Conclusion section of their study:
“We found limited scientific evidence to support the effectiveness of this intervention in the community. Assuming that a high level of compliance with home isolation is possible for symptomatic persons, voluntary home isolation could be a preferable strategy to prevent onward transmission compared with other personal protective measures, which have not shown effectiveness in multiple randomized controlled trials.”
Put in plain English, this review of 50 studies was able to only find “limited” evidence. We will see from my own review that the word “limited” is not accurate. In fact, there was NO evidence in any of the studies that social isolation works with the general population.
Here are my notes from reviewing the observational studies in the the above table:
Quarantine studies
This category included 1 intervention, 5 observational studies and 10 simulation studies. I only reviewed the single intervention and the 5 observational studies. These were references 4 and 18 to 22.
The intervention study used a control group company against an experimental group company where employees could voluntarily stay at home on receiving full pay when a household member showed development of influenza-like illness until days after the symptoms subside. The intervention backfired because many more people in the intervention group got sick by staying home than did not get sick at work due to the absence of the worker. The conclusion was that home quarantine was not a good idea because it actually increase the number of flu victims. None of the 5 observational studies provided evidence supporting quarantine measures other than quarantine of the the actual flu victims.
School Dismissals or Closures
School dismissal refers to the situation where a school campus remains open with administrative staff and teachers present but most children stay at home. School closure is a stricter intervention in which a school campus is closed to all children and all staff.
School closures do reduce flu spreading slightly during a closure. However, transmission returns to the rate it would have been once the school re-opens. Thus, there is not a significant difference in the total number of victims.
None of the reviewed studied had any bearing on the corona virus because all of them assumed that children would be the main carriers of the flu virus. In fact, with the corona virus, there are very few confirmed cases under the age of 18.
Here is a quote from one of the studies:
“There is no consensus on the scale of the benefits to be expected, and recent reviews highlighted the lack of evidence for social distancing measures such as school closure.”
Another study just confirmed the importance of hand washing.
Here is a quote from a 2006 study:
“Ill persons should remain home when they first become symptomatic, but forced isolation and quarantine are ineffective and impractical. If the pandemic is severe, social distancing measures such as school closures should be considered.
https://www.ncbi.nlm.nih.gov/pubmed/16494723?dopt=Abstract
There was one study with actual evidence. It was a comparison of a school closure in Hong Kong one year to when schools were not closed in a different year. The study “ detected no significant effect of school closure on influenza spread in this outbreak.” Here is the link: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(09)70176-8/fulltext#back-bib4
Below is a graph comparing the flu illnesses in the closure year (2007) to the non-closure year (2008):
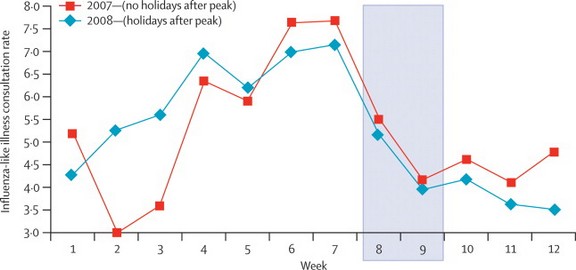
It is pretty obvious that the closure did not effect the total number of infections. Three other studies estimated that reactive school closures had no effect in reducing the total attack rate and duration of school outbreaks, and the spread of influenza (34–36).
Here is a quote from another study which had no real data but argued against school closures: “School closures can also have adverse impacts on ethical and social equity, particularly among vulnerable groups (e.g., low-income families). Extended school closures might increase contact rates in households and other social gatherings (e.g., malls, theaters), with the potential to increase transmission in the community.”
That’s it for the second fake study. Now for the third.
#3 A third study claims to provide evidence that social isolation works On April 6, 2020, another study was published claiming to prove that social isolation policies work – and predicting mass deaths if the social isolation policies are lifted too soon. The study was called Quantifying the Effect of Quarantine Control in Covid 19 Infectious Spread. Here is a link to this study: https://www.medrxiv.org/content/10.1101/2020.04.03.20052084v1.full.pdf
Let’s look at the evidence they provide to back up their claims.
Red flag #1 is that this study is using machine learning. In other words, it is a computer simulation. As I noted above, computer simulations suffer from the problem of “Garbage In, Garbage Out.” But because of the claims they are making, we will still review this study.
Red Flag #2 is that one of their first citations is the discredited 2020 Ferguson report.
Red Flag #3 was their claim that South Korea “adopted drastic generalized quarantine. This resulted in apparent recession of the spread in South Korea.” Their statement is simply false. There was not a mandatory generalized quarantine in South Korea like there was in China.
Red Flag #4 was their claim that the response in the US was “delayed.” (they then claim the delay led to explosive growth of infections and fatalities). In fact, infections and fatalities in the US are much less than in many countries in Europe that implemented immediate lock downs.
Red Flag #5: They claimed that the US is somehow the worst responder in the world. Here is a quote from their shoddily written study: “As of April 2 2020, the United States has the highest number of infected cases (∼ 227k) globally.”
Do you spot the error? They never adjusted for population. At the time, the US was at 30 deaths per million while many countries in Europe were over 100 deaths per million – three times worse than the US in terms of cases per million and deaths per million.
Red Flag #6: Their machine learning model completely ignores the role of our natural immune system in bending the curve of the virus. All effects are attributed to social isolation policies. No attempt was made to isolate the two factors. Therefore, since all gains in their computer model were due to social isolation, they predict that the virus will take off again once social isolation is ended.
In short, they simply ignore our natural immune system. And this is the kind of fake science that is being used to justify locking down the entire US. Wow. There is simply no scientific research that supports any social isolation policies.
That’s it for the third study. Now for our fourth and final study.
#4 This is not actually a study. It is much worse. It is a YouTube video made by a doctor in Texas and viewed by more than 15 million people. My daughter sent it to me and wanted to know what was wrong with it. Here is a link to the 30 minute video: https://www.youtube.com/watch?v=4J0d59dd-qM
Sadly, even though the person making the video is a doctor, he made several basic mistakes indicating he knows very little about the human immune system.
His first mistake was at minute 3 when he said that “because it is a new virus, no one has any immunity to it.” This is not true. While the corona virus is new, it is similar enough to other corona viruses, such as the common cold, that about half of all people exposed to it will not get it because they already have a natural immunity to it.
He also seems to be unaware of the research on asymptomatic carriers – which confirms that for every reported case, there are at least 50 asymptomatic cases (see the video I just posted to my Facebook page).
He is also wrong at minute 4 in claiming that “20% of people who get the corona virus will need to be hospitalized.” What he should have said was 20% of confirmed cases will need to be hospitalized.” (the number is actually 10% of confirmed cases).
But in ignoring the huge number of asymptomatic cases, he makes a fool out of himself. The real percent that will need to be hospitalized is 10% divided by 50 = 2 in one thousand actual cases or one in 500 cases. This makes the corona virus exactly like the seasonal flu in terms of risk of hospitalization (and risk of death).
Again at minute 4, because he ignores the issue of asymptomatic cases, he greatly over-estimates the percent that will need to be in the ICU or on respirators (by a factor of 50).
His conclusion that we do not have enough respirators is simply wrong. In fact, we have at least twice the number of respirators that we will need even when the epidemic is at its peak. Sadly, this doctor simply failed to “do the math.”
He then is wrong in his analysis of how corona virus kills people – as most claimed victims to not actually die from the corona virus.
He is correct in claiming at minute 5 that fatalities are linked to high blood pressure and obesity. He is wrong in claiming that over 40 is at risk. The press reports on this have not been accurate. It is still age 70 that is the huge increase in risk and even age 70 is not a risk unless you have other medical problems such as cardiovascular problems.
He is also wrong in his claim that if a person sneezes and you are within 6 feet, “You have a very good chance of catching it” In fact, we know that it takes a high concentration of the virus to get infected. Mere exposure to the virus does not lead to infection. Even then, you will only catch it if your immune system is compromised in some way. His claims are basically fear mongering on a massive scale. Your actual odds of catching it are well under 10% and your odds of dying if you do catch it are less than one in one thousand.
He then spends about 10 minutes explaining just one of many pathways that people have been killed supposedly by the corona virus replication process. He fails to recognize that many supposed corona virus victims were never even tested for the corona virus and are likely to have died from bacterial pneumonia – which is different from pulmonary edema or viral pneumonia. The differences are important because the treatment for these three medical conditions is different. As just one example, putting someone on a respiratory may not be the best course of action if the respirator increases the pressure in the lungs too much. A better course of action may be supplemental oxygen combined with antibiotics. See the following link for more information on differences in treatment: https://www.ncbi.nlm.nih.gov/books/NBK513286/
At minute 21, he states that 3% of cases will die. Again, because he ignores the research on asymptomatic cases, the real number is 5% divided by 50 which is 1 person in one thousand.
He is correct at minute 24 in saying half the time when people are put on a ventilator, they do not survive. But at least some of this problem is misunderstanding what is happening in the lungs. If the lungs are still healthy, some doctors now believe that there may be other better options and that the ventilator itself might make the breathing problem worse. See for example, Dr. Cameron Kyle-Sidell, emergency room doctor from NYC in this video: https://vimeo.com/402537849
At minute 25, he again makes the mistake of claiming that there are not enough ventilators. This is because he over-estimates the number of people who will need ventilators by at least a factor of 50 to 80. He wants us to “trust him.” But sadly, he failed to research these issues before he made the video.
He then recites case numbers without any research into whether the case numbers or fatalities are accurate. In fact, we have known all along that the case numbers and fatalities are extremely inaccurate for a whole bunch of reasons.
He then states at minute 26 that Italy has a 10% death rate from the corona virus. This is simply ridiculous. But because this guy is a doctor, people will believe that what he is saying is true. In fact, he will be eventually proven to bee wrong. This is why a lot of people no longer trust doctors. It is because too many doctors go public with opinions when they have failed to do any kind of research.
At minute 27, he then talks about doctors dying from the corona virus. I am sure doctors have died. I have seen no evidence that what they died from was the corona virus. Science requires that we demand some actual objective evidence before accepting claims.
He then claims that we will not hit the peak until Mid May. In fact, we now know that the peak was hit about April 20, 2020. So he is off by at least one month. This is why scientific research is important. There is no research that supports a peak of Mid May – much less the peak used in the Ferguson report of Mid-June.
He then uses a doubling ratio of every three days. Research has shown that the doubling period is about every 6 days. So this fear mongering doctor is distorting facts almost with every sentence.
He then at minute 19 claims that because you did not take this seriously, your grandmother is going to die.
In fact, the person who did not take this seriously enough to do any research is this doctor. And because of his fear mongering video, government officials will shut down our economy which will cause 300,000 people. In short, he and the people who listen to them will cause death on a massive scale. All because they failed to do any research and knew nothing about our immune system.
He then claims that “we do not have a treatment for this.” In fact, Vitamins C and D have been found to be effective treatments as have transfusions of corona virus antibodies. Again, he has done no research.
At minute 33, he then falsely claims that we are worse off than Italy or Spain. This is ridiculous. As of April 18, 2020, deaths per million in Italy is 358. Deaths per million in Spain is 409. Deaths per million in the US is 101. The problem in Italy and Spain is three times worse than it is in the US. But because he is a doctor, people will believe him without ever bothering to check out the facts.
The take away from this is first, do not listen to someone simply because they are a doctor. Do your own research. Second. we need to do a much better job teaching doctors about how the immune system works.
The Real Crisis has been Empty Hospitals
Here is a quote from a May 4, 2020 Global Research article:
“Aside from New York, nationally there’s been no health system crisis. In fact, to be truly correct, there has been a health system crisis, but the crisis is that the hospitals are empty. This is true in Florida where the lockdown was late, this is true in southern California where the lockdown was early, it’s true in Oklahoma where there is no statewide lockdown. There doesn’t seem to be any correlation between the lockdown and whether or not the epidemic has spread wide and fast.”
What’s Next?
How can we account for this hard to understand but scientifically proven result that mass gatherings are extremely safe? The answer is in having a better understanding of the extremely complex relationship between viruses and the human immune system. Let’s look at recent studies that are finally shedding some light on what is really going on between humans and viruses (including all strains of flu viruses and cold viruses).